Pain
Conventional Treatments for Spondylolisthesis

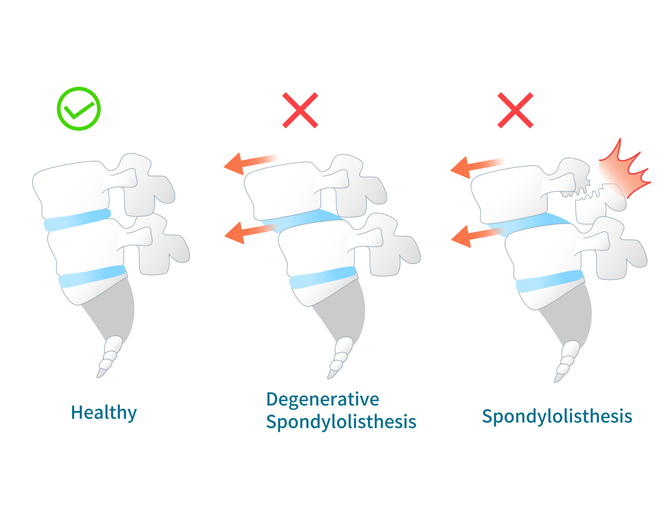
What is spondylolisthesis?
Spondylolisthesis is a medical condition that primarily affects the lower back (lumbar spine); however, it can also occur in the mid to upper back (thoracic spine) or neck (cervical spine). The body has 33 stacked vertebrae that form the foundation of the spine. Spondylolisthesis occurs when a vertebra slips forward (anterolisthesis) or backward (retrolisthesis) onto the vertebra underneath it, which may lead to nerve compression.
Conventional treatments for spondylolisthesis
Spondylolisthesis treatment is dependent on pain severity and vertebral slippage. The goal of nonsurgical treatment options is to reduce pain and stimulate the vertebrae to go back into place. Any contact sports should be avoided during the healing process. Conventional treatments for spondylolisthesis include medicine, injections, physical therapy, bracing, facet ablation, and surgery.
Medications
- NSAIDs. Over-the-counter medications, such as ibuprofen or naproxen, may reduce pain. Stronger NSAIDs may be prescribed if over-the-counter medication fails to ease pain. Examples include ibuprofen and celecoxib.
- Muscle relaxant. This type of medication can help ease back pain that results from muscle spasms. Examples include baclofen or methocarbamol.
- Anticonvulsant. If a slipped vertebra is pressing on a nerve and causing nerve pain, an anticonvulsant medication may be prescribed. Examples include topiramate and gabapentin.
- Opioids. If pain is severe and other medication does not help, opioids may be prescribed. Examples include codeine or morphine.
Injections
Options for injection therapies for spondylolisthesis include the following:
- Epidural steroid injections can precisely transport steroidal medications to specific spinal regions. It helps decrease pain and increase functionality by reducing joint inflammation. Steroid injections are not likely to help joints that are severely damaged. They are not recommended more than once every three to four months.
- Facet joint injections involve a small amount of local anesthetic and steroid medication that is injected into one or more facet joints that are causing pain. A local anesthetic provides immediate pain relief, while a steroid medication reduces inflammation and provides long-lasting pain relief.
Physical therapy
Physical therapy is often prescribed to treat spondylolisthesis. The physical therapist will target areas of weakness with exercises that strengthen abdomen and back muscles. Posture and movement awareness is taught to prevent future damage.
Bracing
A brace can be prescribed to stabilize the spine and limit movement. Bracing allows fractures to heal and is most regularly used with children.
Facet ablation
Also known as radiofrequency rhizotomy, facet ablation uses energy waves to stop the nerve’s from transmitting pain. It is not a long-term solution, since the benefits typically last between nine months to three years. Physician therapy is recommended during the period of pain relief.
Surgery
It is generally recommended to try non-surgical procedures before resorting to surgical treatment options for spondylolisthesis. However, in some cases of spondylolisthesis, surgery may be necessary.
A lumbar interbody fusion (LIF) is the typical surgical procedure for spondylolisthesis. The approaches of the vertebral fusion include anterior (front), posterior (back), and transforaminal (side). The goal of LIF is to decompress pressure on the spinal nerve, correct spine alignment, and stabilize the spine.
During decompression, the surgeon will remove anything causing pain by pressing on a nerve. The type of decompression is dependent on the structure that is compressing the nerve. Nerve compression associated with spondylolisthesis can occur from the following:
- Bulging or herniated disc — A discectomy removes the part of the disc that is compressing a nerve.
- Narrowed foramen — A foraminotomy makes more room for the nerve to pass through the foramen (a passageway for spinal nerve roots). Vertebral realignment is also completed if needed.
- Central Spinal Stenosis — A laminectomy will remove the lamina (the flattened part of the vertebral arch) if there is not enough room for the spinal cord or spinal nerves as they travel through the spinal canal.
- Lateral recess stenosis/Gills fragment — A facetectomy removes a Gill fragment, which is a part of the facet joint that breaks, causing nerve compression.
Following decompression, the spine will be fused for stabilization and the surgeon will fill the gap with a bone graft. The bone graft can come from the individual or a donor. Synthetic substances that promote bone growth can also be used. A surgeon may use screws, rods and cages to support the spine as the vertebrae fuse together.
Minimally invasive vs open surgery
In many cases, a lumbar interbody fusion can be performed as a minimally invasive surgery. This type of surgery uses several small incisions instead of one large incision. Minimally invasive surgery has less blood loss, and less cutting of the muscles, ligaments and tendons. This results in a shorter recovery time and hospital stay. Many times, a combination of minimally invasive and open surgery are completed together, which is referred to as "mini open.”